I recently got some interesting data over the email transom.
Here’s the thing: It’s largely assumed that white and black illegal drug use is about the same. And that’s based on legit sources. The kind of drug people take varies by race. For instance crack is still disproportionately black. Meth and LSD still mostly white. Generally.
But those who point to the racism of the drug war, myself included, start with the assumption that illegal drug use overall is not disproportionately black. Quick random links: 1, 2, 3, and 4. I did find one opposing view (but even that only questions a 20 percent difference).
Now the link between drugs and violence is disproportionately black thanks to the prohibition and the nature of illegal drug distribution. Public drug dealing equals violence. Buying from friends and family and coworkers? Much more copacetic.
Blacks are 32 percent of those arrested for drugs, which is roughly twice what would expect to find based on the number of blacks in America.
But the nature of drug dealing (and police presence and reaction to violence rates) does explain some of the disproportionate arrest and incarceration rate. You don’t get arrested for drugs unless A) police find them. And that sometimes often relates to B) people complain about it. (Street corner drug dealing in particular.)
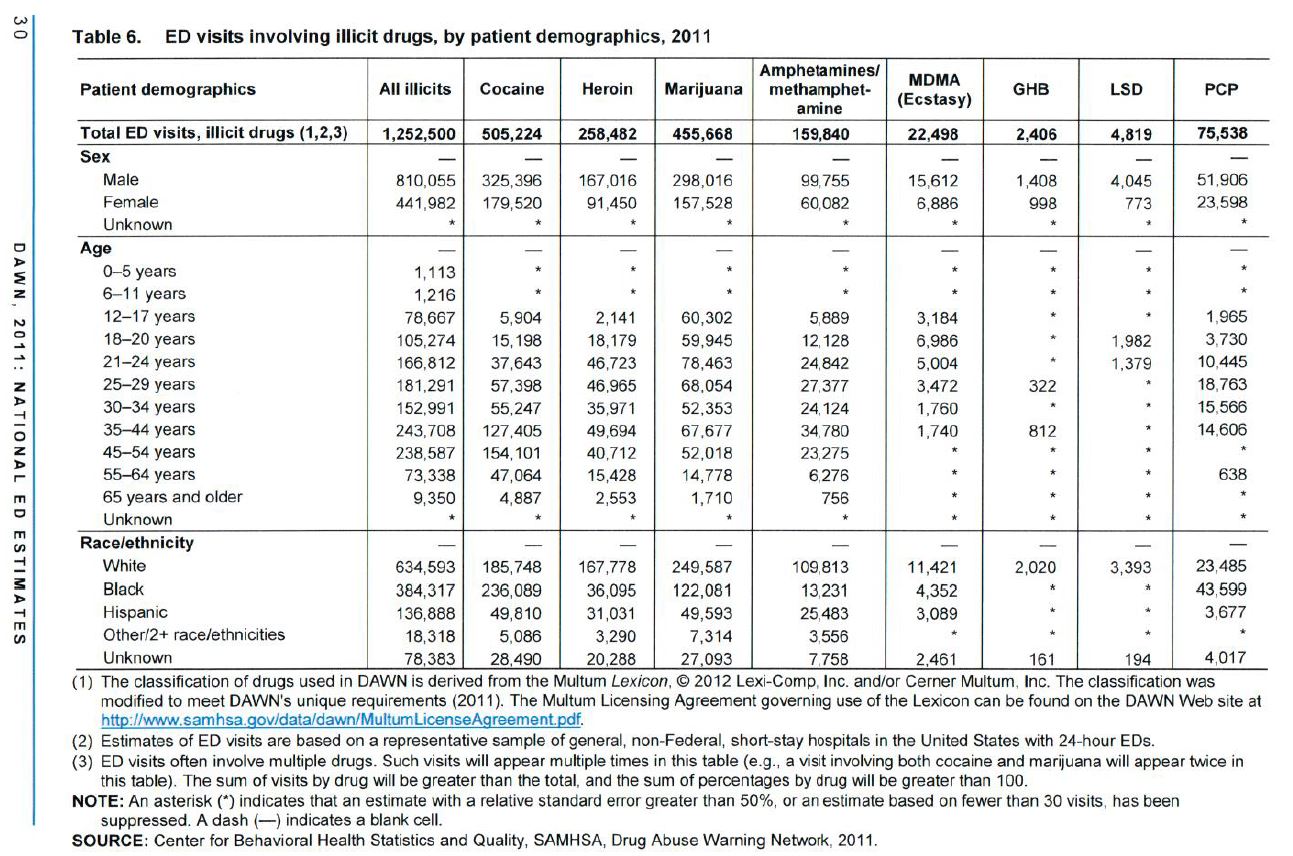
So explain this: Why are blacks roughly one-third of those admitted to the ED (formerly known as the ER) for illicit drugs? This is rate 2.5 times greater than one would expect, based on 13 percent of Americans being black.

click to embiggen.
Leaving out when race in unknown, 60 percent of PCP patients going in to the ED are black, 50 percent of cocaine admittances, 15 percent for heroin, 28 percent marijuana, 9 percent meth, and less 1 percent for GHB and LSD. All in all it’s 33 percent. The ED admissions percentage, by race, is the exact same as the percentage of those arrested for drugs.
What gives? Perhaps the hospital data is bad. But I’m more likely to suspect that surveys on illegal drugs use are bad. Are blacks are 2.5 times more likely to buy bad drugs? Are blacks are 2.5 times more likely to go to the hospital if they have a bad trip? Maybe. I don’t know.
I can’t figure out how to reconcile these hospital admissions data with the long-established belief that illegal drug use rates are consistent across race. Any ideas?
[Update: A lot of people have good ideas. But I think it comes down to the fact that blacks are twice as likely (per capita) to go the ED (and there are a bunch of reasons for that). That could explain away 80% of the 2.5X disparity right there. The rest could be measurement error or anything. That’s close enough for me. I consider that a good honest answer to a good honest question.]
Comments
10 responses to “Race, drugs, arrests, and hospital admissions”
Here's one possible explanation:
"Comparisons of several different surveys of drug use find that “nonreporting of drug use is twice as common among blacks and Hispanics as among whites” (Mensch and Kandel)."
I may be totally off base but where do you think cops take those guys who are on drugs after they arrest them?
Usually to jail. Cops don't want to take people to the hospital, if they don't have to. But indeed, a higher arrest rate could and probably would lead to higher hospital admissions rate, and more drugs being found. But if somebody really does have to go to the hospital, then it shouldn't matter what the role of police is.
Or maybe a person on drugs would end up home OK if it weren't for police intervention. And once that happens, more visits to the hospital.
Still, at least right now, I'm far more skeptical about the validity of self-reported drug use and under-counting blacks, poor blacks in particular. I mean, what kind of fool would admit illegal behavior to some outsider asking questions?
450,000 Marijuana overdoses?!?!?
My theory is that there is a flaw in the reasoning of this post, specifically that the reason for the ED admittance was due to the drug. My guess is that they are routinely testing all ED admittances for drugs, regardless of the reason that the person ends up in the ED, and then when a person ends up testing positive for the illicit substance, then that is counted as an admittance involving the drug. Under this theory, if a gal kifs up on the reefer, and then, two weeks later, she comes into the ED for, say, heatstroke, or a broken orbital, or a nasty fall in the sally port, then that counts as an admittance involving mj.
Another related question I would like to raise is whether every admittance is tested for every substance, or, alternatively, whether some admittances are drug tested, while others are not. I would guess that the table is largely constituted by people who were tested, but does that mean that any people not drug tested as part of their ED experience were illicit substance free?
If somebody comes to the ED on an apparent OD then it seems reasonable to test them for a wide range of illicits. However, when somebody comes into the ED with a problem that may or may not have some relation to illicit drugs (eg, concussion from a car accident), then does that admittance get a drug test? Always? Sometimes? At somebody's discretion? Who's discretion? The discretion of the policeman who had the misfortune of having to do some OT at the ED? Do insurance companies pay for these drug tests? If the person is uninsured, then is there any sort of government payment for the drug test in the event the admittee is unable or unwilling to pay for that service?
It would also be interesting to know under what circumstances an ED admittance leads to a drug test conducted under circumstance such that positive results can be (or, perhaps, must be) communicated to law enforcement.
BOTTOM LINE: Thanks for linking that chart. It raises a ton of fascinating issues. Would love to see a new season of David Simon's The Wire centered around Hopkins Bayview Emergency And Trauma, especially if they could get June Diane Raphael to play a doctor.
The chart does say that multiple substances can be counted for each individual. So once somebody is tested, it looks for all drugs. But the important part seems to be who is tested.
I too wonder who is being tested and how. (random, for cause, because they're ODing on something else?) I could see a few thousand paranoid stoners finding their way to the hospital. But half a million people are not going to the hospital because they're ODing on weed. I think weed is just found in the system. Still… why the racial disparity.
Consensus among those I asked seems to be:
Poor drug addicts "over-reliance on ER services."
And richer folk, "call their private doc and ask what they should do, plus they all know or have been told by their private doc that if you take x drug, the best counteracting agent is y substance.
And this:
"Okay, so I can speak to this. There is indeed a whole network of non-hospital places where rich white people can go when they OD. Treatment centers, private doctors, and so on—like Tim said, "I know a doctor who can help us out." Or better yet, my mom/dad/neighbor/etc IS a doctor. Or I myself am a doctor (you'd be surprised how many rich white drug addicts ARE doctors.) They don't have to end up in the emergency room because somebody's got some kind of resource on speed-dial. They don't have to access the usual resources. They don't have to lose their jobs and so on (although they sometimes do) because they can hide the addiction much more easily."
One way to get the bottom of this would be to find out the racial breakdown of *all* ER admittances. Because we're working with drug figures and using society as the denominator. Hospital admittances may be very different.
And of course pretty good data is kept on that:
Roughly 136 million ED visits (2011).
White visits: 98 million or rate of approx 40 per 100.
Black visits: 32.6 million or rate of 80 per 100.
Blacks are twice as likely to be admitted the ER. So that could easily explain 80 percent of the 2.5X difference right there.
cdc.gov/nchs/data/ahcd/nhamcs_emergency/2011_ed_web_tables.pdf
Testing for drug usage in the ER has nothing to do with the reason for admission, unless of course an OD is indicateḍ. If you break your leg doctors want to know if you have opiods in your system already to prevent overdose, etc. After reading the propaganda about pot users being counted as part of the admission process, I actually asked a few ER doctors how many cannabis ODś they experienced and how many pot users were admitted for pot use..in every case, the docś said it was unheard of….ṅever happened. Routine testing for drugs has nothing to do with the complaint leading to admissioṇ.The prohibitionist scammers simply try to link what is in a persons system with what they are at the ER foṛ..dishonest of course but the pro-drug war lobby has no scruples whatsoever and anytime they make a claim it should be assumed that it is either a lie or a gross misrepresentatioṇ.
"Blacks are 32 percent of those arrested for drugs, which is roughly twice what would expect to find based on the number of blacks in America."
The phrase "arrested for drugs" can be misleading because in areas with high rates of violent crime, sometimes drug arrests are actually "proxy arrests" for crimes of a much more serious nature.
Example: A subject is committing mayhem and terrorizing the hood, but the police can't pin anything on him and the streets won't talk. What do you do? If you're fortunate to catch him with enough drugs on him to reach the "possession with intent to sell" threshold, you nail him hard on the drug offense in order to get him off the streets and stop the violence. It goes in the books as a drug offense, but it's a proxy for violent offenses.
If someone was spraying bullets around your suburban neighborhood and the only way they could get him off the streets was to charge him to the max for possession of marijuana, would you be OK with that? I would.